Colon volvulus (CV) denotes the twisting of a segment of the colon around its mesenteric axis. This rotation can cause blockage of the bowel lumen and restrict blood flow, potentially leading to ischemia or perforation of the affected colon segment. CV ranks as the third most common cause of large intestinal obstruction, following colorectal cancers and complicated sigmoid diverticulitis. The incidence of CV varies globally, with higher prevalence in regions termed the “volvulus belt,” which includes all mos over the world contaning Asia, America, Europe and many more. This distribution may be linked to dietary, lifestyle, and genetic factors contributing to the development of a redundant colonic segment susceptible to volvulus [1].
Volvulus can occur in any colonic segment with sufficient redundancy to twist upon itself, most commonly involving the sigmoid colon (60–70\% of cases) and the cecum (25–40\% of cases). Other colonic segments are rarely affected, but when involved, the clinical presentation can be atypical, making diagnosis more challenging. A particularly rare and complex form of this condition is double colon volvulus, where two separate segments of the colon twist simultaneously, presenting significant diagnostic and management challenges. Understanding the pathophysiology, epidemiology, and clinical implications of CV is crucial for healthcare professionals, especially in high-prevalence areas. This case report follows the SCARE criteria [2-4].
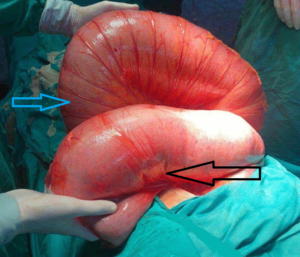
A 50-year-old female, a non-smoker and non-alcoholic with no chronic diseases, who had undergone an appendectomy via the McBurney procedure, presented with a 7-day history of complete bowel obstruction, a markedly dilated abdomen, absence of defecation or gas passage, no specific abdominal pain, and no nausea or vomiting. Upon examination, her vital signs included a pulse of 80 beats per minute, blood pressure of 100/60 mmHg, and normal body temperature and respiratory rate. Her abdomen was severely distended with generalized tenderness and reduced bowel sounds; a rectal exam revealed an empty rectum without any intraluminal mass. Emergency laboratory results showed a White Blood Cell Count (WBC) of 8000/mm³, hemoglobin of 13.0 g/dL, and normal serum sodium and potassium levels. An abdominal X-ray revealed grossly distended large bowels with air-fluid levels, and a CT scan showed an extremely distended large bowel. A laparotomy was performed, revealing cecal and sigmoid colon volvulus and an intensely distended colon without signs of perforation or ischemia, though with parietal thinning. Abdominal exploration indicated the absence of all colon ligaments. A colectomy was not performed due to the patient’s family’s refusal; instead, abdominal drains and closure were performed. Postoperatively, the patient resumed bowel movements about 4 hours after the operation and was discharged after 2 days.

Colon volvulus (CV) involves the twisting of a redundant colon segment around its mesentery, which can cause luminal obstruction and compromise blood supply, potentially leading to ischemia, gangrene, and perforation. The global prevalence of CV varies, with higher rates in the “volvulus belt,” including regions in Africa, South America, Russia, Eastern Europe, the Middle East, India, and Brazil. In these areas, CV accounts for a significant portion of intestinal obstructions, ranging from 13\% to 42\%, compared to 10–15\% in the USA and Europe. Double colon volvulus cases are rare.
Risk factors for colon volvulus are multifaceted, including lifestyle, anatomical, and medical factors. A low-fiber diet can lead to chronic constipation, increasing the risk of sigmoid volvulus. A sedentary lifestyle also raises the risk of constipation and subsequent colon volvulus. One potential risk factor for sigmoid colon volvulus is the length of the rectum and sigmoid, with the longest lengths observed in African patients. A mobile cecum, a congenital abnormality where the right colon fails to fuse to the posterior parietal peritoneum, is a possible cause of recurrent right lower abdominal pain, misdiagnosed acute appendicitis, and cecal volvulus.
The main clinical presentation of CV includes sudden, severe, crampy abdominal pain, significant abdominal bloating or distension, nausea, and vomiting. If the volvulus leads to bowel ischemia and necrosis, signs of peritonitis, such as fever, tachycardia, and tenderness on palpation, may develop.
Imaging studies, particularly CT scans and abdominal X-rays, can show the “whirl sign” indicative of volvulus or the classic “coffee bean” sign in sigmoid volvulus cases.
Initial management of sigmoid volvulus typically involves sigmoidoscopy with rectal tube application, although surgical treatment has a higher survival rate and should be considered if there are signs of peritonitis, unsuccessful conservative management, or to prevent recurrence. Colonoscopy-assisted sigmoidopexy is effective in preventing recurrence, while cecopexy without resection can be performed for viable cecum walls before standard treatment (right hemicolectomy) in cecal volvulus cases.
Mortality rates are influenced by age, with patients over 75 at higher risk, coexisting cardiopulmonary diseases, and late admission. However, there is no evidence linking the type of intestinal volvulus with increased mortality risk.
Colon volvulus, characterized by the twisting of the colon around its mesenteric axis, presents significant diagnostic and management challenges, especially in regions with high prevalence. The condition predominantly affects the sigmoid and cecum, with risk factors including dietary habits, anatomical variations, and lifestyle factors. This case highlights the importance of prompt diagnosis and tailored management strategies to prevent complications such as ischemia and perforation.
The successful management of our 47-year-old patient with both sigmoid and cecal volvulus, without perforation or ischemia, underscores the necessity of individualized treatment approaches. Despite the absence of colectomy due to family refusal, the patient experienced a favorable outcome with rapid postoperative recovery.
Understanding the multifaceted risk factors and clinical presentations of colon volvulus is crucial for healthcare providers. Emphasis on early detection, appropriate imaging studies, and timely intervention can significantly improve patient outcomes. Future research should focus on refining diagnostic criteria and management protocols to further enhance the care of patients with this complex condition.